Deinstitutionalization
Empty hallway of an abandoned psychiatric hospital with sunlight coming through broken windows.
The Dive
Deinstitutionalization refers to the process, beginning in the 1950s and accelerating through the 1970s, of closing large state-run psychiatric hospitals and relocating patients to community-based programs. Advocates believed this approach would be more humane, less isolating, and supportive of patients’ dignity and independence. At first, the vision promised a more compassionate future for mental health care.
The scale of change was enormous. In 1955, more than half a million Americans lived in state psychiatric hospitals. By the 2010s, only about 37,000 public psychiatric beds remained, representing a more than 90 percent reduction. Experts agree that while some hospital closures were overdue, the sudden lack of available care created new problems.
The federal government tried to support this shift through President John F. Kennedy’s 1963 Community Mental Health Act, which aimed to fund local clinics. However, the money for long-term operations never fully arrived, leaving a gap between ideal plans and reality. Medicaid rules further restricted funding for psychiatric hospitals, and later political changes cut back federal support even more.
Court cases such as O’Connor v. Donaldson (1975) emphasized that people with mental illness could not be confined without cause, reinforcing civil liberties. While these legal decisions protected rights, they did not guarantee services. Many people who once would have been hospitalized instead ended up without treatment or housing.
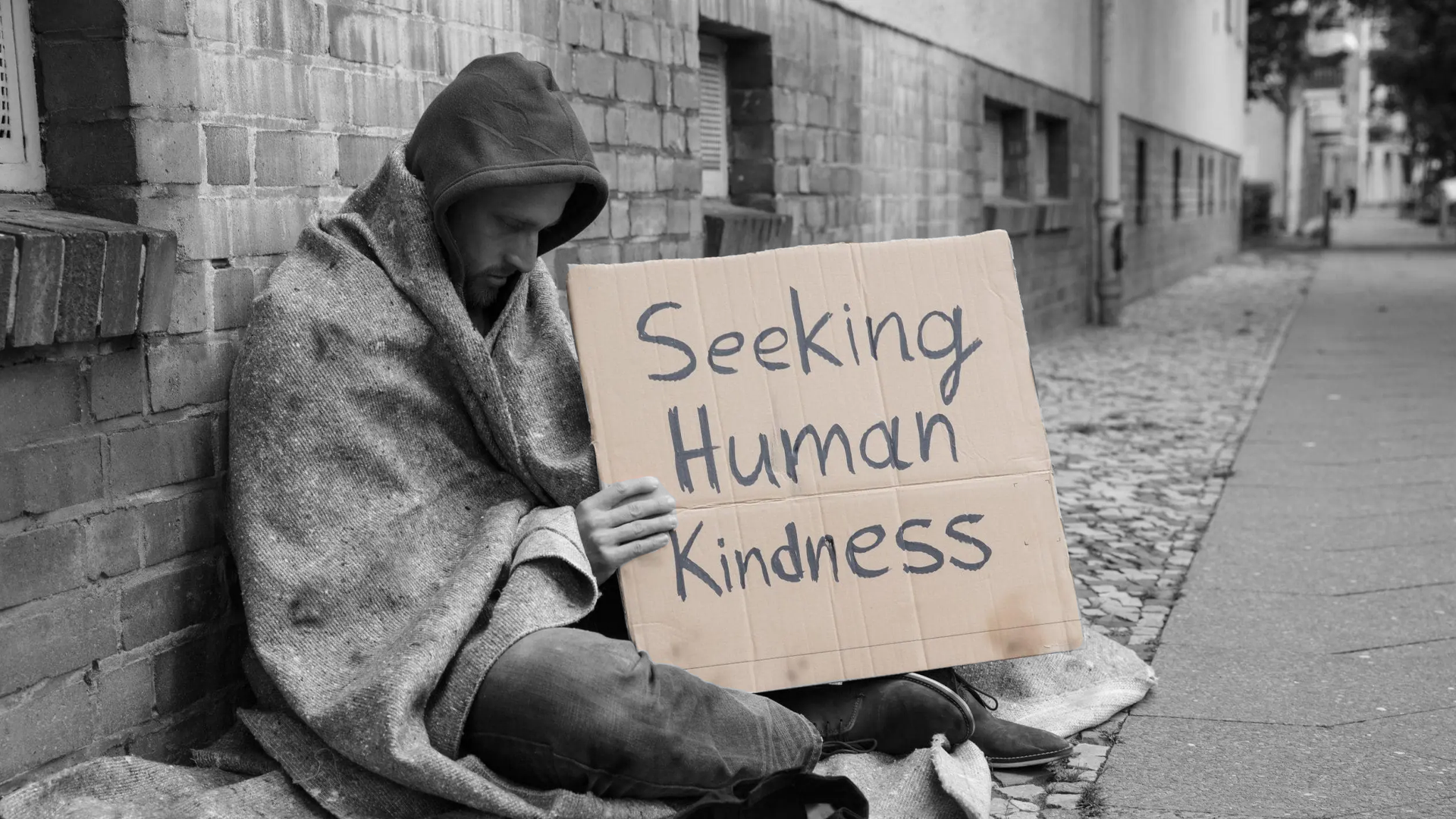
By the 1980s, the results were visible in American cities: rising homelessness and increased incarceration of people with mental illness. Scholars describe this as ‘transinstitutionalization’—meaning that instead of ending institutional care, society simply shifted it from hospitals to jails and prisons.
The consequences continue today. Homelessness remains closely linked with untreated mental illness and substance use disorders. Jails have become, by default, the largest providers of mental health care in the country. Emergency rooms often struggle to house psychiatric patients because of the shortage of long-term beds.
While deinstitutionalization began as a movement for justice and compassion, the lack of investment in community programs left many people vulnerable. True reform requires building the services originally promised: supported housing, crisis treatment centers, and robust outpatient care.
The story of deinstitutionalization is a reminder that good intentions alone are not enough. To truly honor human dignity, societies must match ideals with resources, ensuring that liberty is paired with real, accessible support.
Why It Matters
Deinstitutionalization reveals the tension between ideals and outcomes in American history. It teaches us that protecting freedom without providing services can lead to abandonment rather than empowerment. Understanding this history helps us recognize why mental health, housing, and justice systems are deeply connected today—and why solutions must address all three together.
?
What were the goals of deinstitutionalization, and why did supporters believe it was a better system?
How did legal changes like O’Connor v. Donaldson affect the rights of people with mental illness?
Why did the lack of community services create new challenges after psychiatric hospitals closed?
In what ways did deinstitutionalization contribute to modern problems like homelessness and incarceration?
What kinds of solutions could better support people with serious mental illness today?
Dig Deeper
An overview of the challenges facing the U.S. mental healthcare system, including issues created by deinstitutionalization.
A look at modern policy debates about balancing liberty and treatment in mental health care.
Related

What Is Community?
Community is more than just a place on a map—it’s people, relationships, and the daily actions that tie our lives together.

Understanding Triggers
Triggers aren’t just reactions, they’re messages from our past asking to be understood.
Birthright Citizenship: The Right of the Soil and the Right of the Blood
From English common law to the Fourteenth Amendment, birthright citizenship has shaped who belongs in America — and who is excluded.
Further Reading

Stay curious!